Anterior Cruciate Ligament and Medial Cruciate Ligament Injuries During Skiing and Snowboarding
Primarily ski and snowboarding injuries tend to affect the Anterior Cruciate Ligament (ACL) and Medial Cruciate Ligament (MCL) with rare occurrence of a Posterior Cruciate Ligament (PCL) injuries. This post will go through the ACL and MCL injuries, grades, and treatment. Please note that everyone’s instance is different and no one person is the same. This is general information only and is not patient specific. If you would like more information regarding these injuries please feel free to contact myself or follow up with your regular physiotherapist/physical therapist.
From my experience Anterior cruciate ligament (ACL) and the Medial cruciate (MCL) injuries tend to occur more frequently in skiers than in snowboarders.
For alpine skiers, the occurrence is amongst the highest in sport, with female skiers being reported to have a significantly higher rate of injury. Usually if there is solely an MCL injury it tends to be that of a grade one or two, whereas if the ACL is implicated it generally means the ligament has ruptured. This places increased strain onto the menisci, particularly the lateral meniscus (more so than the medial meniscus) as well as the MCL producing further injury into these as well as other structures within the knee complex.
What is the Medial Collateral Ligament (MCL)?
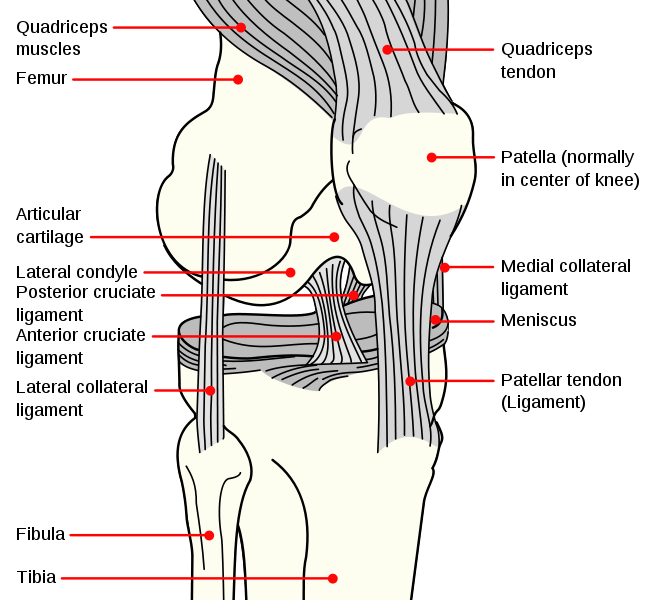
The MCL is located on the medial side (inside) of the knee. It is one of the 4 main ligaments of the knee that help enhance its function and stability. Essentially it restricts excessive movement of the knee to prevent the medial aspect of the knee opening up.
Most MCL injuries on the mountain tend to be either grade one or grade two tears and are treated non-operatively with physiotherapy. A grade one tear produces pain on assessment but there is no laxity (instability) observed, there is some tenderness over the MCL but there is no instability seen. A grade two tear produces more pain on assessment with 5-10mm of laxity plus increased swelling than that of a grade 1. If a grade three tear occurs it usually is less painful as the ligament is completely ruptured but shows significant instability and swelling over the MCL.
What is the Anterior Cruciate Ligament (ACL)?
The ACL is located deep and in the middle of the knee. It essentially goes from the posterior aspect of the femur to the anterior aspect of the tibia. It works to resist anterior movement of the tibia as well as rotational loads.
Injuries to the ACL come in 3 grades as well. In a grade one tear the individual reports a minor pain and swelling, they report the knee still feels stable. The don’t report it to give way during activity and on assessment there is a firm end feel (meaning to the physiotherapist or physician performing the assessment that the ligament is intact). Grade two injuries results in the ligament being partially torn (not a full rupture) with haemorrhaging occurring. There is tenderness and a moderate amount of swelling. They complain of some instability with some occurrences of the knee giving out during activity. On assessment, there is increased anterior translation (movement forward of the tibia) of the tibia with a firm end point that may be painful due to the partially torn ligament being pulled on. A grade three, like the MCL refers to a complete rupture of the ACL. It is reported to be tender but it does not necessarily feel painful as the ligament has been torn in half. Everyone is different in the amount of swelling that is seen, some people have minimal and some people have a lot and the knee feels unstable and gives way. there is no end point on assessment and there usually is bleeding into the joint space present.
In relation to skiing most stories about the mechanism of injury go like this (this refers to a more frequent reports but not all instances of ACL injuries on the mountain):
One mechanism involves the skier catching the front inside edge of the ski resulting in the tibia rotating externally. The skiers momentum continues forward, the lower leg is abducted (moving away from the body) and externally rotated producing a significant torque on the knee.
Another common mechanism occurs when a skier is landing a jump, and the centre of gravity is positioned to far back. The tail of the ski lands first, this leverages the tibia anteriorly via a force transmitted through the top of the boot and creates an anterior drawer effect resulting in an isolated ACL injury.
Thirdly, if a off-balance skier sits with the weight back on the skis and catches an inside edge on the snow, this results in a sudden internal rotation of the knee that continues to flex. The back of the ski then provides the torque required to rupture the ACL.
Treatment
Please note the below is only a general initial guide, and everyone is not the same. For more specifics please contact myself or your usual physiotherapist for more detailed information regarding your circumstances.
Initially the aims of treatment are as follows:
- Control the swelling (REST: rest, ice, compress, elevate)
- Early weight bearing
- Initiate sufficient quadriceps muscle activation
- Increase the range of motion of the knee
- For MCLs, pending on their severity, a period of immobilisation is required to enable the ligament to heal and to enhance recovery. This in turn essentially provides greater strength and stability down the road.
- Graded return to strength training program.
- Proprioception training, (the ability to feel how the body is positioned in space) . Try to think of balance activities.
- Stationary bike training
- Pilates
- Movement retraining and education
- Stretching
- Jumping and agility training (further down the line and is patient specific)
- Surgery may be required for either ACL/MCL injuries pending on the individuals circumstances.
As always, if you are looking for a consultation or treatment, do not hesitate to get in touch. Next week’s post will look into Meniscal injuries. In the meantime, have fun shredding the slopes and be safe!
Cheers,
The Nomadic Physio